
La relation entre développement économique et mortalité infantile
Otto Kolbl
The question is fundamental: to what extent does economic development, as measured by GDP growth, lead to a reduction of mortality, for example of infant mortality? The Western media do not talk much about this topic; recent Western academic publications on this topic all arrive at the same conclusion: there is a relationship, but it is not very strong.
Actually, when the data analysis is done correctly, based on the most reliable data available, the result is quite surprising: if we take all the countries for which reliable data is available (n=187) and exclude countries which massively export oil or mining products (n=30), the Pearson correlation coefficient between GDP per capita purchasing power parity (GDP PC PPP) and infant mortality rate (IMR) is -0.92, which is huge. This indicates that there is a very strong relationship between infant mortality and economic development: higher GDP means a lower infant mortality; the inverse relationship is indicated by the negative sign of the correlation coefficient. By taking the square of the coefficient, if we assume a causal relationship between GDP and IMR, we find that 85% of the whole variance of IMR across the world is explained by GDP levels alone.
The interactive chart below shows GDP per capita purchasing power parity (GDP PC PPP) on the x-axis and the infant mortality rate (IMR) on the y-axis, all data for 2015. The axes are logarithmic, with a constant added before the log transform in order to get a symmetric distibution (one of the preconditions of the Pearson correlation coefficient). GDP PC PPP is widely considered to be the best indicator of standard of living. The infant mortality rate indicates how many babies die in their first year of life out of 1000 babies born alive; it is considered to be a good indicator of the performance of the health care system in general. The menu "More information" provides more details about the variables and the sources. Hovering over and then clicking on one of the data points provides comprehensive information about the data sources used for this point and about various calculations as well as about the scales used for the axes.
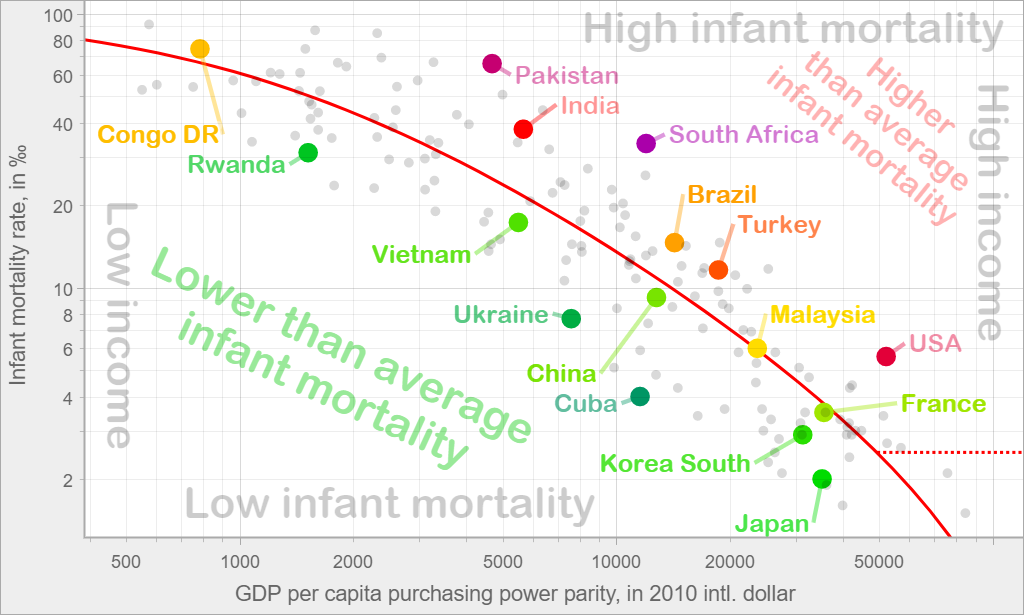
One thing becomes clear at the first glance: no low-income country has come even near the values of IMR which the industrialized countries can offer to their citizens. All countries with a GDP below 1000$ have got an IMR above 40‰. All the countries below 3000$ have got an IMR above 30‰. Conversely, all the countries above a GDP of 30,000$ have got an IMR below 6‰. This clearly shows that in the long term, economic development will certainly lead to fewer babies dying in their first year of life, and it is the only way of achieving this objective.
The red diagonal line represents the linear regression between the two variables. In other words, this is the line for which the sum of the squares of the vertical distances between the line and the various points is minimal. It allows us to calculate the average IMR which we would expect for a certain GDP level, based on the IMR achieved by the various countries for their respective level of GDP. If a country is significantly below the line, it has provided a better-than-average survival chance for the babies born there. If a country is significantly above the line, we can consider that its achievements in the field of health care are questionable, unless we find another explanation for its poor performance.
The difference between actual IMR and the expected value calculated through the linear regression line, in combination with data about the population and crude birth rates, allows us to calculate the number of babies which were saved by a better-than-average performance of the health care system, or the number of babies which could have been saved by an average performance. All this data is available for each country in the tooltip which appears when the mouse hovers over one of the data points. When you click on the point, the tooltip is frozen and you can get even more detailed information by a click on a button.
With the menu item "Customize - Select countries", you can select the countries to highlight without having to search through the 100+ dots on the chart. In the timeline below, you can select the year to display; the available timespan is 1950-2015.
The second chart below shows why countries which massively export oil or mining products have been excluded from the first chart and from the calculation of the correlation coefficient and the linear regression. These countries are displayed as empty circles, whereas the countries from the previous chart are displayed as discs.
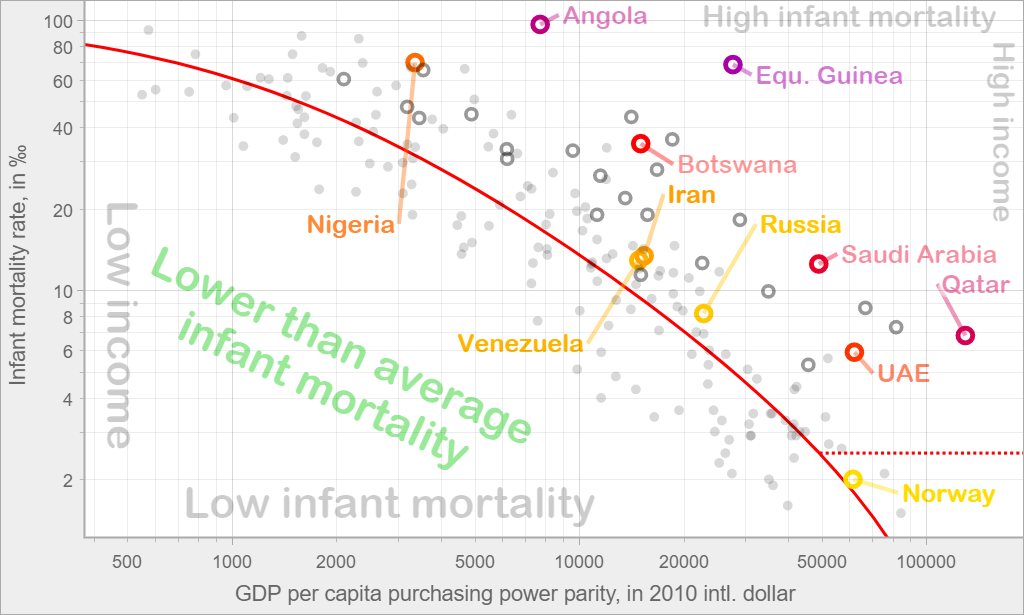
Except for Norway, none of the oil and mining exporting countries have got a better-than-average healthcare system. Why do countries with large income from natural resources have such underperforming health care systems? This is probably linked to the interests of the ruling elite. In most countries, if the elite wants to increase their income, they must motivate the workforce to give their best. In oil-rich countries, the money flows into the state coffers without any effort by the local workforce. How much each person gets from this "blessing" only depends on how many people have to share it among themselves. It is therefore in the interest of the ruling elite to keep as many people as possible isolated in the countryside, without infrastructure, education, Internet access and healthcare, so that they don't claim their fair share.
The only way of achieving social progress in these countries is therefore to inform the local population about the extent of the wealth which the elite keeps for themselves instead of using it for the good of the population. However, providing solid information to the local population requires research like the one presented here, based on solid data, which can measure precisely the extent of the theft and the number of human lives it claims. Unfortunately, academic research in this field is totally inadequate.
The bibliography below shows all the articles found on this topic in an extensive search in 2012; it will be updated shortly. All these articles present some research about the relationship between economic development and infant mortality, and all of them arrive at the conclusion that there is some relationship, but that it is not very strong. Since a simple correlation will immediately show the extent of the actually very strong relationship, how is it possible that each single recent article arrives at the opposite conclusion?
Most of the articles set up complex models with multiple explaining variables. There are several reasons why they miss the very strong relationship between GDP and IMR:
- Several of them "forget" to do the log transforms of the variables, which are necessary for the variables to satisfy the preconditions of statistical methods like Pearson correlation, linear regression, etc. Without an adequate log transform, the correlation is much lower ( -0.57 instead of -0.92).
- Some of them focus on the short-term relationship between increase in GDP and decrease in IMR. This relationship is not very strong because in the short term, economic liberalization which leads to economic growth often has a negative impact on the health system. However, in the long term, IMR will more and more be impacted by GDP levels. Actually, the Pearson correlation coefficient between the two variables has had a tendency to increase, from -0.77 in 1950 to -0.92 in 2015, after a peak of -0.94 in 1998.
- Some articles use GDP figures based on official exchange rates instead of purchasing power parity, which decreases the relationship.
- One of the projects works only with data about wealthy countries. If you look for a relationship between one variable and another one, but you take only a small fraction of the variance on one of the variables, it is not surprising that you find no significant correlation.
Such an accumulation of methodological problems in all the recent articles on this topic cannot be the product of chance. Based on extensive research in this and many other fields, my best guess is that each article is the result of a long series of decisions, each one being unconsciously impacted to a certain extent by ideological bias, i.e. the wish to get a result which fits into some commonly accepted academic weltanschauung. The key elements of this weltanschauung which are relevant to this topic can roughly be described as follows:
- Academics tend to see themselves as countervailing powers to the economic and political elites. In particular, they consider that they defend higher humanist and immaterial values whereas the economic elite is characterized by greed and the political elite by a compulsive quest for power. Having to admit that in the long term, only economic development as measured in its crudest form (GDP growth) can reduce the number of babies dying in their first year would deal a devastating blow to their self-image.
- Another basic assumption of the Western academic world seems to be the moral and intellectual superiority of the West over all other civilizations. The first chart above directly shows the way to a method of evaluating the effort of each country to provide health care to its population as required by the fundamental UN texts relating to human rights ("the reduction […] of infant mortality" "to the maximum of its available resources", see the International Covenant on Economic, Social and Cultural Rights, articles 12 and 2). If we look at the efforts of each country in relation to its available resources, it is obvious that many developing countries will get a better evaluation than some industrialized countries. This seems to be unacceptable to many Western academics.
- Previous research has revealed that the Western media, to some extent under the influence of the academic system, tend to amputate the human rights of certain aspects, among others the obligation by the states to make sure that everybody can enjoy some basic services like health care and education. This can explain why the whole topic of infant mortality has never really been a priority of academic research in human science outside of the narrow field of medical research. Obviously, those who do medical research do not take economic growth into consideration.
- A fourth explaining factor is that academic researchers tend to spend their lives in ivory towers with limited contact to the outside world. If you just talk with a few people from developing countries who have seen misery and extreme poverty with their own eyes or know about it through the narrations of family members, the strong relationship between economic development and the reduction of infant mortality becomes obvious. Of course, Western academics are in close contact with academics from developing countries, but this does not really help them to leave the ivory tower: in most developing countries, researchers working in human science tend to come from families of intellectuals who have generally had a privileged life for generations. In industrialized countries too, academics or their families have never had to struggle with access to health care or education.
- A last factor is the way in which academics tend to see governance, namely as something which is determined by policies, policy changes and political reforms. They consider that the more influence academics get in the decision making processes, the better the outcome. Therefore, having to admit that by far the biggest factor determining infant mortality has got nothing to do with health policy is definitely a problem. An even bigger problem is probably the fact that if we consider the residual of the above-mentioned linear regression (i.e. the remaining variance after the impact of GDP has been excluded), many of the countries which do well are countries with various forms of authoritarian political regimes where academic freedom is not at its best (e.g. communist regimes), whereas many of the most liberal political regimes perform quite poorly.
- To sum it all up: it would be a terrible embarrassment if we had to admit that the Chinese Communist Party was right to prioritize economic development, because in the long term, it is the only way to massively reduce mortality...
All these are only hypotheses which can explain why the extremely strong relationship between economic development and infant mortality has been ignored and even negated by the academic community, but none of these hypotheses have been confirmed by specific research; they are all open for discussion. However, in the topic of the present article and many other fields, academic research has been more than problematic, and these issues must be addressed one day.
The present article is more an overview of my findings rather than a comprehensive presentation of the results. More detailed articles will follow about each aspect of the problem.
Bibliography
Berkeley, D. and J. Springett (2006). "From rhetoric to reality: Barriers faced by Health For All initiatives." Social Science & Medicine 63(1): 179-188.
Biggs, B., L. King, S. Basu and D. Stuckler (2010). "Is wealthier always healthier? The impact of national income level, inequality, and poverty on public health in Latin America." Social Science & Medicine 71(2): 266-273.
Charles, K. (2009). "A Century of the Infant Mortality Revolution." Retrieved 2015/10/22, 2015, from http://charleskenny.blogs.com/weblog/files/histinf.pdf.
Clark, R. (2011). "World health inequality: Convergence, divergence, and development." Social Science & Medicine 72(4): 617-624.
Elola, J., A. Daponte and V. Navarro (1995). "Health indicators and the organization of health care systems in Western Europe." American Journal of Public Health 85(10): 1397-1401.
Ensor, T., et al. (2010). "The impact of economic recession on maternal and infant mortality: lessons from history." BioMed Central Public Health 10(727).
Griffey, B. (2011). "The ‘Reasonableness’ Test: Assessing Violations of State Obligations under the Optional Protocol to the International Covenant on Economic, Social and Cultural Rights." Human Rights Law Review 11(2): 275-327.
Macinko, J. A., L. Shi and B. Starfield (2004). "Wage inequality, the health system, and infant mortality in wealthy industrialized countries, 1970–1996." Social Science & Medicine 58(2): 279-292.
Moore, S., A. C. Teixeira and A. Shiell (2006). "The health of nations in a global context: Trade, global stratification, and infant mortality rates." Social Science & Medicine 63(1): 165-178.
Randolph, S., S. Fukuda-Parr and T. Lawson-Remer (2010). "Economic and Social Rights Fulfillment Index: Country Scores and Rankings." Journal of Human Rights 9(3): 230-261.
Stuckler, D., S. Basu and M. McKee (2010). "Drivers of Inequality in Millennium Development Goal Progress: A Statistical Analysis." PLoS Med 7(3): 1-13.